Introduction
Delirium is an acute neurocognitive condition affecting up to half of patients in palliative care units.1,2 The condition involves acute and fluctuating changes in attention, awareness, and cognition,3 with common precipitants being dehydration, infection, and psychotropic medications.4,5 Delirium increases risk of falls and pressure injuries, prolonged admission and physical and cognitive deterioration.2,6 Patients find delirium symptoms and associated emotions such as fear and anger difficult, and carers and clinicians experience distress witnessing them.5,7,8 Timely recognition and response to delirium symptoms depend on knowledgeable clinicians, routine structured screening, and effective teamwork.9 Yet delirium is under-addressed in many hospital settings.10
Clinical care standards for delirium are in place in some countries.9,11 In Australia, the Delirium Clinical Care Standard (‘Delirium Standard’) covers delirium prevention, early diagnosis, treatment and concomitant care via eight quality statements and 12 quality indicators, with patient-centredness the overarching principle.9 This Standard has become the key quality framework for delirium care in Australian hospitals.
There are gaps in how palliative care units in Australia have implemented the Delirium Standard, with areas for improvement including systems, practice, clinician understanding, and provision of information for patients and carers.12 Delirium prevention may be possible for around a third of patients, but prevention strategies are under-utilised.13,14 Managing delirium is challenging in this setting because its reversibility near the end of life can be uncertain, addressing all causes may not be possible for dying patients, and there are no interventions proven to safely relieve delirium symptoms.15–17 Palliative care clinicians also use antipsychotics and benzodiazepines for delirium more often than clinicians working elsewhere.18
Implementing the Delirium Standard would improve the safety and quality of delirium care in palliative care units. We plan to support this implementation by integrating the Standard with a national symptom monitoring program, the Palliative Care Outcomes Collaboration (PCOC). PCOC aims to improve patient and carer outcomes in palliative care using patient and proxy reported measures.19 These measures include the PCOC Symptom Assessment Scale, a numerical rating scale of 0 (absent) to 10 (worst possible) for patients’ level of distress from common symptoms such as pain and fatigue.20 The measures are routine and inform clinical care. Six-monthly PCOC national and site-specific reports support review and benchmarking of clinical outcomes.21 Observational data indicates that PCOC is feasible, valid and effective in improving palliative care outcomes.20,22,23
The current PCOC collection has no delirium measure. We designed the ‘Monitoring Delirium in Palliative Care’ (MODEL-PC) study to inform such an addition.
MODEL-PC study objectives are to:
-
Collaboratively develop a new delirium monitoring system (Text box 1) for palliative care units that integrates the Delirium Standard, PCOC methods, and patient, carer and staff perspectives.
-
Pilot the new delirium monitoring system and measure implementation, effectiveness and systemic utility (feasibility, acceptability and appropriateness) outcomes to determine whether it can be more widely tested and used to meet the Delirium Standard in palliative care units, +/- via PCOC.
Methods
Design
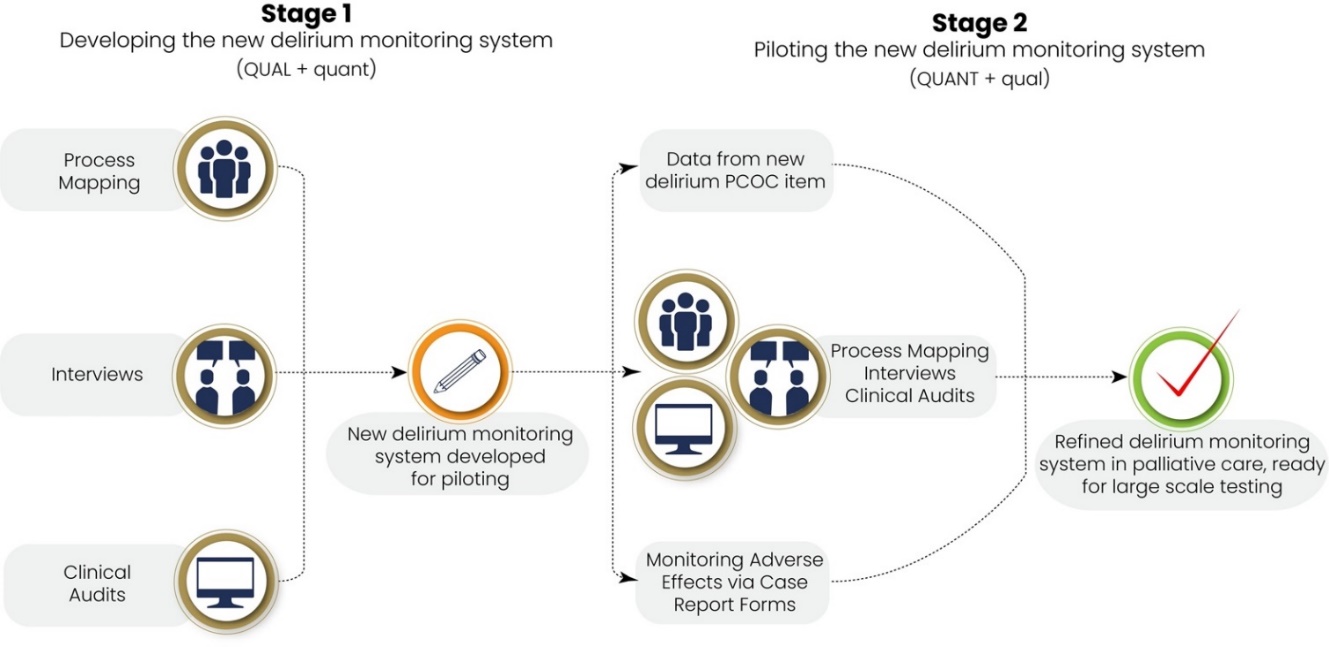
This is a two-stage multicentre exploratory sequential mixed methods implementation study. The new delirium monitoring system will be developed in stage 1 then piloted in stage 2 (Figure 1). ‘Exploratory’ signifies initial prioritisation and positioning of qualitative methods/data (‘QUAL/quant’) over quantitative (QUANT/qual), an appropriate sequential ordering when developing a new process or measure and our rationale for using mixed methods.24 The MODEL-PC study sits within the “adaptation, preparation, feasibility and piloting” stage of implementation research, as articulated in the Standards for Reporting Implementation Studies (StaRI) Statement.25

Setting
Palliative care units (PCUs) in Australia are multidisciplinary services specialising in prevention and relief of suffering for inpatients with life-limiting illness and their carers. Four PCUs from metropolitan New South Wales, Victoria, and Western Australia will be included. Patients in this setting have a mean age of around 75 years26; and around 65% die during admission, with delirium occurring more often for this group compared to discharged patients.
Participants
Participants include adult patients, carers, and staff of participating PCUs.
Eligibility
Patients eligible for an interview will be adult (aged 18 years or older), admitted to a participating PCU, English speaking or have a health care interpreter available, experienced delirium in the preceding week, and willing and able to consent and participate. Patients in the terminal phase (last days to hours of life) will not be asked to participate in an interview. Patient’s medical records will be audited if they are aged 18 years or older and admitted for more than 24 hours. PCOC data will be obtained from all PCU inpatients in stage 2.
Carers eligible for an interview will be an adult family member or friend of an admitted patient, present when the patient had delirium in the preceding week, English speaking or with a health care interpreter available, and willing and able to consent and participate. Carers will not be asked to participate in an interview if the patient is in the terminal phase, although those who previously consented and wish to continue may do so.
Staff eligible for process mapping and interviews will be adults employed in a clinical or unit-level managerial role who are willing to consent. Interview participants must have cared for a patient with delirium in the preceding week.
Data collection and entry
Site research staff will collect data, with senior clinicians contributing to clinical auditing. Most patient items are routinely collected in clinical practice. Research staff will enter data into a study-specific REDCap database.27
Stage 1 data collection includes:
-
Process mapping, a systematic, collaborative and rapid method to map PCUs clinical policy and processes against the Delirium Standard.28 Researchers will facilitate between 1-3 sessions with key staff from each PCU, record discussions and enter data in REDCap (Supplementary file 1). Results will be presented to key PCU staff for verification before finalisation.
-
Clinical audits of patients’ medical records (N=240, 60 per PCU) to obtain data on documented delirium practices and outcomes. The audit tool aligns with the Delirium Standard and contains predominantly Yes/No responses plus optional free text on application/relevance for individual patients (Supplementary file 2).
-
Semi-structured interviews (N=80, 20 per PCU: 5 patients, 5 carers, 10 staff) will align with the critical incident technique (CIT), a research method that gathers detailed first-hand reports about satisfactory and unsatisfactory execution of a task in order to refine it.29,30 The focused, brief and storytelling CIT interview method is ideal for unwell patients and hard-pressed carers and staff. Site research staff will be trained in CIT, with the interview schedule (Supplementary file 3) designed to obtain recounts of delirium care in the preceding week. Staff participants will be additionally asked how recalled incident/s might inform practice alignment with the Delirium Standard and PCOC.
Stage 2 data collection will mirror stage 1, with additional measures, different time points, and nuances reflective of stage 2 objectives, as follows:
-
Process mapping: end of the stage, to allow sufficient time for change in delirium care.
-
Clinical audits: monthly results rapidly fed back to PCU teams.
-
Semi-structured interviews: additional focus on receipt or delivery of the new PCOC measure/s and other changes in delirium care.
-
New PCOC delirium measure/s: completed by clinical staff and collected by research staff from every medical record. PCOC data will include completion (Yes/No), reporter (patient, carer and/or clinician) and scores.
-
Adverse events, to capture potential study harms and/or the new delirium monitoring system to patients, carers, staff or organisations.
Data items are outlined in Supplementary file 4.
Implementation strategies
MODEL-PC study implementation strategies include:
-
Overall alignment with key principles for successful health systems integration as identified in a systematic review by Sutor et al,31 with six explicitly applied (Text box 2).
-
At the end of stage 1, outcomes will be presented to study investigators, key PCU staff and other stakeholders, including in an online workshop where those involved will co-design a new delirium monitoring system that addresses the Delirium Standard, articulates the new PCOC measurement for delirium, and specifies activities, tools, time points and persons required. Within these prerequisites, PCUs will be free to vary how they apply the new monitoring system and meet the Delirium Standard e.g., choice of validated screening tool.
-
Stage 2:
a. Two-week run-in for new PCOC measurement when research staff will seek clinical staff feedback on the process.
b. Data feedback of monthly audit results to key PCU staff, who will asked to disseminate these to their wider team.32
c. Staff training in the Delirium Standard and PCOC measurement, tailored to/by PCUs based on stage 1 and emerging results and preferences for mode e.g., one-on-one, inservices.
Outcomes
Stage 1 and 2 outcomes are outlined in Tables 1 and 2.
Sample sizes
For clinical audits, each PCU is considered an independent site with probable low (<2%) current complete compliance to the Delirium Standard (based on previous audits at two sites). To detect changes in estimated proportion of compliance for eligible patients (determined by a decision tree incorporating delirium present yes/no and deceased vs discharged) of at least 10% between stages with an assumed intracluster correlation coefficient (ICC) = 0.01, alpha = 0.05 and power = 0.8 will require 120 clinical audits per site (60 per stage), thus an overall total of 480.
PCOC delirium items will be collected from approximately 1,000 patients; with the mean of 2.2 palliative care phases34 per admitted patient, this will potentially give >2000 data entries for analysis, providing at least 2.5% level of precision in estimating frequency of delirium-related events in the overall study population, with 95% confidence and assuming a conservative 35% likelihood of delirium diagnosis during admission.
Qualitative interview sample sizes will be determined from number of incidents rather than participants, as per CIT. Adequate data collection will be when an additional 100 critical incidents identify no more than two additional relevant behaviours, which we will determine at 50, 150 incidents, etc. in each stage. Using this calculus, we anticipate needing at least 80 participants in each stage (N=160). A minimum quota of 40 patient interviews will address their under-representation in qualitative studies of delirium in palliative care.12
Analyses
Quantitative data analysis will use descriptive statistics (means and standard deviations, medians, interquartile ranges, frequencies) to summarise participants’ characteristics and implementation study outcomes. Where appropriate, standard tests for normality will be conducted and outliers assessed for numerical variables. In stage 2 clinical audit data analysis, a multiple logistic regression model will be used to assess predictors of achievement versus non-achievement of the Delirium Standard. Results will be compared across study sites and potential reasons for disparities in patient characteristics, admission patterns and outcomes explored. Missing data will be assessed for any non-random patterns.
Qualitative data will be recounted incidents with an antecedent, a clear description of the incident, and an outcome, congruent with CIT.29,30 We will perform thematic content analysis framed against the Delirium Standard with inquiry focused on its feasibility, acceptability and appropriateness in the PCUs.35,36 A sub-set of investigators with qualitative analysis experience will perform initial analysis and develop preliminary themes and sub-themes, then present these to the full investigator team for refinement before finalisation.
Data integration through triangulation of quantitative and qualitative summary data will occur at the end of each stage and reported in narrative and diagrammatic summaries and joint displays.37
Ethical considerations
Recruitment, enrolment and consent
For interviews and process mapping, we developed brief and simplified participant information sheets and consent forms with 13-point font and lay language resulting in a Flesch Kincaid reading ease score of 8.3 (equivalent to 8th grade student standard) for the patient version (Supplementary file 5). Site research staff will recruit eligible people, rather than site investigators who may have clinical or managerial responsibility for some who asked to participate. People eligible for interviews or process mapping will be given sufficient time to make participation decisions. Research staff will endeavour to avoid undue research burden on patients and carers by prioritising their individual needs and wishes over recruitment targets. Patients will be free to consult with trusted others and undertake the interview in their presence if they wish. Participants will confirm their consent in writing. Research staff will record participants’ names and details in a participant master log, assigning each person a unique participant identification number (PID). Research staff will be trained in study-specific consent and interview processes and experience of delirium from patients’ perspectives.8,12
Waiver of consent to audit medical records and use PCOC data was approved by the Human Research Ethics Committee (HREC), with patients or their proxies able to opt out. An opt-out approach was ethically justified because inclusion of routinely collected clinical data on delirium care and outcomes carries no more than low risk to patients, project validity requires most eligible patients be included, potential study benefits outweigh risks, and data will be maintained in accordance with relevant security standards.38,39
Potential risks and their mitigation
The MODEL-PC study involves patients who are highly dependent on medical care, near the end of life, experiencing distress, and many with cognitive impairment. We will minimise potential risks to patients, carers, staff, participating organisations and the project as outlined in Table 3.40
Dissemination
Outputs will include the study protocol, stage 1 interview findings, stage 1 clinical audit results, stage 1 mixed methods integration, stage 2 interview findings, stage 2 PCOC results, and overall project mixed methods results, and corresponding conference presentations.
Discussion
Delirium is a serious but under-addressed condition in Australian palliative care units, estimated to occur for around 22,000 patients annually.1,45 The MODEL-PC study will, for the first time, obtain patients’ perspectives of delirium and delirium care and their levels of distress in this setting.12 Patient recruitment processes align with the MORECare capacity statement, which focuses on maximising individual autonomy, allowing sufficient time and resources for participation, and recruitment strategies that anticipate and address patients’ varied capacities, including fluctuations in individual patients.46 This ‘supported decision-making’ approach privileges the person with a disability as the decision-maker and affords them equal rights, respect and necessary support for decision-making, without abuse or undue influence.47,48
Alignment and interlinking of the Delirium Standard with PCOC monitoring methods increases the likelihood that PCU staff will adopt the study processes, given the potential for measures and efficiencies that may help them to meet a hospital accreditation requirement. MODEL-PC study findings will inform the development of a funding proposal for a definitive implementation trial, as well as quality improvement in delirium care in palliative care settings in Australia and other jurisdictions with a delirium standard. The study will build understanding of how PCOC data can drive quality delirium care in PCUs and may inform future PCOC data linkage projects. It will provide PCOC and all registered palliative care services across Australia with exemplars of delirium care to use when they train clinicians in use of PCOC delirium items, thus aiding research translation. It will also aid service-level quality improvements and national surveillance and monitoring, which will be useful in helping to determine whether the Australian standards for delirium are being addressed in palliative care services.23
Acknowledgements
We thank Mr Jonathon Lennon for his expertise and assistance as a project officer in the initial phase of the study; and Ms Clare Johnston, Research Development and Grants Coordinator, for her support in the grant application and management.
Author Contributions
AH, MA, CJ, GW, PM, AC, RC, JO, MS, CV, MP, IF, SB, PL conceptualised and developed the study proposal and submitted it for grant funding in 2020. Full protocol development was led by AH with contributions from the remaining authors. NVO led the tailoring of the full protocol into this protocol manuscript. All authors approved the submitted manuscript.
Ethics statement
This research was reviewed and approved by the St Vincent’s Hospita Human Research Ethics Committee (HREC) (approval number: 2022/ETH00110) on 27 May 2022), with Cross Institutional Ratification by the University of Notre Dame Australia HREC (reference number: 2022-096S) on 13 July 2022.
Funding sources
This research is funded by a National Health and Medical Research Council (NHRMC) Ideas Grant (2021/GNT2010701).
Declarations of Interests
PL and SB receive an Academic Protected Time Award from the Department of Medicine, (Blinded for review).
Investigators AH, GW, PM, PC, KB, JO and MS have clinical and/or academic appointments at participating sites.
Progress statement
Stage 1 data collection is complete, with analyses underway. One site withdrew from the study at the end of stage 1 due to complete closure of the hospital. Stage 2 data collection started at the remaining three sites in January 2024. The number of stage 2 audits per site will be adjusted to obtain the 240 required, pending ethical approval of this amendment.