INTRODUCTION
Delirium is an acute, and often preventable medical condition characterised by acute onset, fluctuation, inattention, disorganised thinking, and altered level of consciousness.1 Delirium affects more than 2.6 million hospitalised adults annually in the United States (US).1 Despite its high prevalence, up to 60% of the time, delirium is under-recognised by healthcare professionals.2 Under-recognition can negatively impact patient outcomes, such as increased mortality, morbidity, and financial cost. Patients may require an extended hospitalisation, up to 5-10 days.1 This extended length of stay contributes to higher inpatient healthcare costs of $81 billion annually.3 The mortality risk of patients with delirium increases up to 3-fold the year following diagnosis compared to patients without delirium.4
Kim and colleagues5 recognised assessment as essential in delirium management, driving prevention and early detection. The Confusion Assessment Method (CAM) tool and its adapted versions are commonly used due to their high sensitivity and specificity when used with a structured formal cognitive assessment.6 Continued research recognises that appropriate use of the CAM does require specific training, and operationalisation of the tool can be subjectively affected by nursing experience and attitudes,7 suggesting facilities already using the CAM may need to evaluate the current state of nursing education and the efficacy of its use. Lack of time, staffing, and interprofessional collaboration make routine delirium assessment and implementing delirium management methods difficult, regardless of the screening tool being used.8
The COVID-19 pandemic has exacerbated these existing challenges. Obregon-Gutierrez and colleagues9 recognised that care left undone was a fundamental consequence of the pandemic, causing care to be highly prioritised where essential, with psychosocial and time-consuming activities all receiving lower priority. Delirium has not been accurately prioritised in recent years, despite evidence suggesting an increase in prevalence and mortality, particularly amongst the COVID-19 population.10,11 As such, limited literature examines delirium assessment and the use of evidence-based interventions to mitigate delirium post-pandemic. To address this knowledge gap, the Delirium Point Prevalence Survey was conducted on World Delirium Awareness Day (WDAD), March 15, 2023, to assess worldwide delirium prevalence, structures, processes, and barriers to implementing interventions to mitigate delirium. Forty-four countries and 1,664 units participated in the WDAD study, two of which were our facilities. To better understand the delirium practice and for future quality improvement, we performed a sub-analysis for our two hospitals. Thus, the primary aim was to assess delirium assessment and recognition for patients aged 18 and over among acute care nurses. The secondary aim was to summarise delirium-related protocols, pharmacological and non-pharmacological interventions, and barriers to implementing delirium prevention and treatment, and report qualitative findings of delirium care.
METHOD
Design and Setting
This is a sub-analysis of a prospective, international prevalence survey conducted on WDAD, an annual international day to increase awareness of delirium amongst healthcare professionals, patients, and caregivers.12 Fourteen units at two hospitals: a 652-bed Level-1 tertiary research and academic medical centre and a 207-bed community hospital participated in the WDAD Prevalence Study. Of 11 General Units, seven belong to the community hospital; 4 remaining were from the tertiary hospital. Two High Acuity Units were from a community hospital, and 1 was from a tertiary hospital. General units include medical-surgical, neurology, and orthopedic units, whereas High Acuity Units include step-down and intensive care units (ICU). Approval was received from the Advocate Health Wake Forest University Institutional Review Board (Protocol # IRB00092271).
Participants and Data Collection
Twenty Clinical Nurse Leaders (CNL) from all specialties at two hospitals were invited to complete a web-based survey during the WDAD; 11 (55%) completed the survey. The WDAD Prevalence survey contains 39 “select all that apply” questions assessing the characteristics of respondents, hospitals, units, structures, delirium prevention and management processes, and barriers to implementing delirium evidence-based strategies (Online Supplemental Table 1). In addition, three open-ended questions asked for recommendations for delirium care and future research. To answer the survey questions, these CNLs must have reviewed the unit census and electronic healthcare record (EHR) of patients aged 18 and older at 8 A.M (+/-4hrs) and 8 P.M (+/-4 hrs) on March 15, 2023, to identify the number of patients on the unit, the number of CAM assessments, and positive CAM screening. A patient was defined as having delirium if their EHR documentation reflected at least one occurrence of a positive CAM. All surveys had to be returned to the study team by March 17, 2023, or were excluded. Permission was granted from the international study team to perform this sub-analysis.
Statistical Methods
Categorical survey data were reported as numbers and percentages. Comparative analysis between the two-unit groups (General and High Acuity) was performed using Fisher’s exact test. Continuous data associated with delirium assessments were assessed for normality, and either an unequal sample t-test or Wilcoxon rank-sum test was performed as appropriate to the data. Means and standard deviations were reported. Radar graphs were generated to visualise the Non-pharmacological treatment and Barriers against implementation data.
Data for the variables for Non-pharmacological prevention and treatment, Pharmacological treatment, and Barriers against implementation and/or use of evidence-based strategies are… were assessed and grouped by the variable designating unit type. Percentages were created where the denominator was the number of patients present in their respective units at the AM and PM times indicated on the survey, and the numerators were patients assessed positive by CAM; creating four variable types: AM Patients Assessed Percentage, PM Patients Assessed Percentage, AM Patients Positive Percentage, and PM Patients Positive Percentage. All data were analysed by Stata 17 (College Station, TX: StataCorp LLC) and p<.05 was considered statistically significant.
Results
Patient Assessments
For the tertiary hospital, 137 patients were present on the unit at 8 A.M, 70 (51%) CAM assessments were documented. At 8 P.M of 137 patients, 64 (47%) CAM assessments were performed. At the community hospital, of the 191 patients on the unit at 8 A.M, 154 (81%) CAM assessments were documented, and at 8 P.M, 168 patients were present on the unit, 130 (77%) CAM assessments were documented. Among CAM assessments, positive CAM screening was 2% and 3% (5 CAM assessments at 8:00 A.M. and 8:00 P.M.), respectively. The overall average number of patients assessed for delirium was higher in the morning (AM: 17.5 vs. PM: 14.5), though when stratified by unit type, this pattern was not found in the High Acuity Unit (AM: 10.7 vs. PM: 11.3). There were no significant differences between the unit types in percentage of patients either assessed for, or positive for delirium in either AM or PM (Table 1). However, while not significant at a p<.05 level, the average AM percentage of patients positive for delirium in the General Units trended towards a much lower than average AM percentage of patients positive in the High Acuity Units (General: 0.35% vs. High Acuity: 7.4%, p=.066).
Interventions
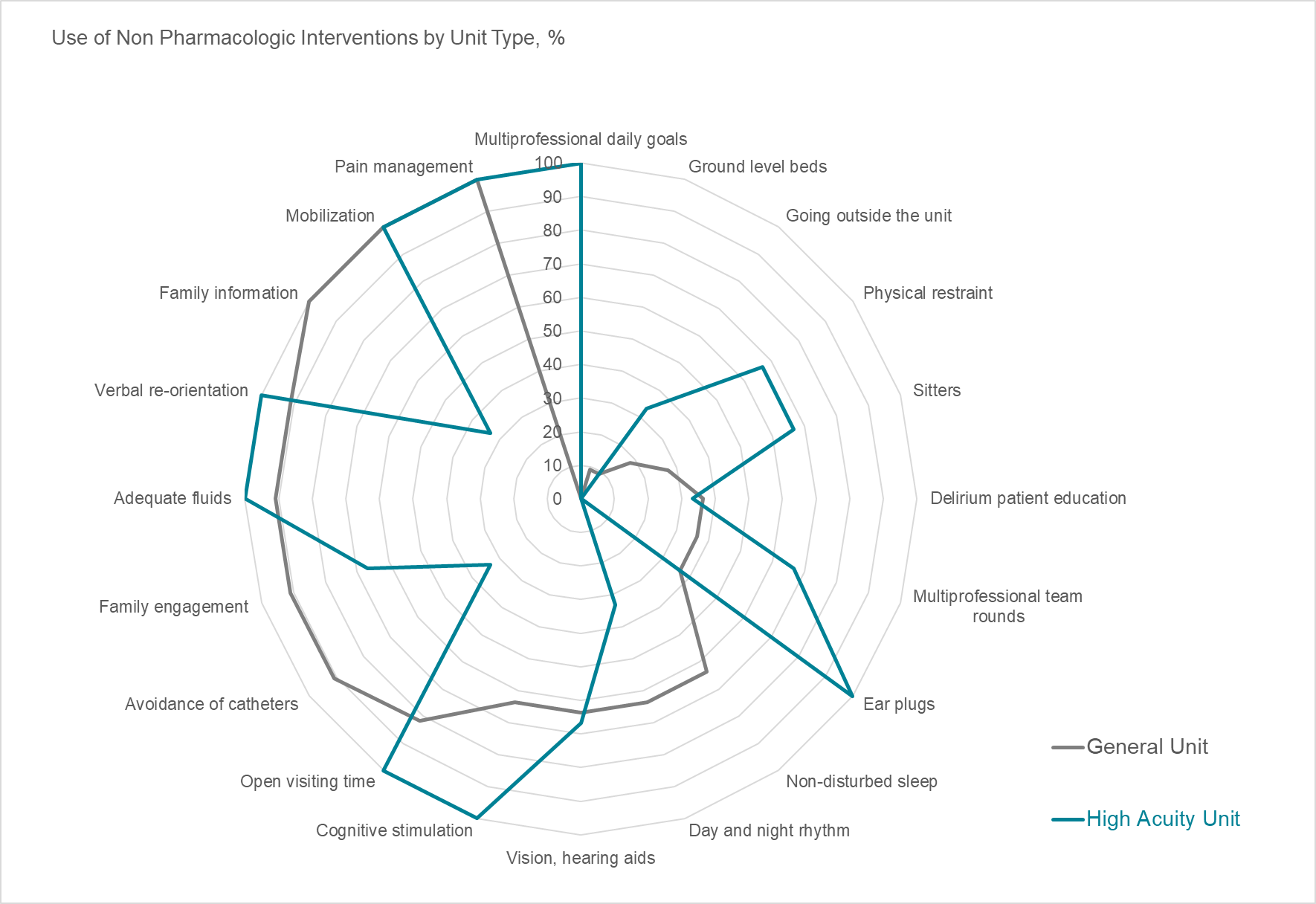
There was a significant difference in the use of multiprofessional daily goals between the two-unit types as a non-pharmacologic intervention for delirium (General: 0% vs. High Acuity: 100%, p=.003) (Online Supplemental Table 2). The General Units reported family information, mobilisation, pain management, avoidance of catheters, family engagement, adequate fluids, and verbal re-orientation at frequencies greater than 90%. The High Acuity Units also reported mobilisation, pain management, adequate fluids, and verbal re-orientation at high frequencies; however, the difference from the General Unit was they also reported open visiting times, cognitive stimulation, ear plugs, and multiprofessional daily goals at high-frequency utilisation (Figure 1). As for pharmacologic interventions, there were no significant differences between the two unit types (Table 2).

Barriers
The High Acuity Units reported “Patients who are difficult for assessment” as a barrier significantly more than the General Units (General: 9.1% vs. High Acuity: 100%, p=.011) (Table 3). The General Units reported a lack of knowledge about delirium and a lack of awareness in frequencies above 90%, and the High Acuity Units also reported these barriers in high frequency, with the addition of shortage of personnel, communication gaps between professionals, and patients who are difficult to assess (Figure 1).
Qualitative findings: Recommendations for delirium care
The survey respondents recommended frequent delirium education, focusing on how to use the CAM tool to increase accuracy. One respondent wrote, staff needs more education on CAM scores. Current scoring may not be appropriate/accurate. Additionally, non-pharmacological interventions such as providing vision and hearing aids, day and nighttime rhythm, multidisciplinary rounds, and patient education are essential in preventing and managing delirium. However, as shown in Figure 1, these interventions are seldom being provided, which may be due to a lack of time and resources. A participant wrote, non-pharmacological interventions can be effective but can take more time. Most units are also not stocked with activities for patients. Participants also suggested leveraging the EHR to increase delirium assessment by linking the delirium assessment admission checklist, or shift required actions; otherwise, CAM is not assessed regularly. Based on the participant’s perspective, integrating this simple reminder will help nurses remember to assess and document delirium in the EHR. Overall, the survey respondents expressed motivation to do the right thing for their patients, as a healthcare provider, I am motivated to promote awareness and education of delirium. However, staff will need support such as enhancing EHR tools, access to delirium prevention supplies, receive continuing delirium education, and ensure adequate staffing.
DISCUSSION
Results revealed that for the two hospitals, delirium assessment compliance was higher in the mornings than at night. This may indicate a need for education and auditing with real-time feedback to promote practice change for night shift nurses. Understandably, the goal is to avoid waking patients to assess them for delirium; however, with appropriate planning, delirium assessment can be performed near the beginning of the shift before bedtime.
The General Units identified a lower percentage of positive CAM assessments than the High Acuity Units. This finding could be related to the need for staff training to ensure that the assessment and documentation are done correctly for follow-up purposes. Education should include the current assessment compliance rates and the devastating effects of delirium. Identifying the why behind this potentially life-saving assessment could positively impact practice change. Additionally, staffing resources could positively impact assessment compliance.
The High Acuity Units used more non-pharmacological interventions than the General Units, such as open visiting times, cognitive stimulation, ear plugs, and multi-professional daily goals. This finding suggests the need for more resources such as interprofessional collaboration, ear plugs, and tools for cognitive stimulation, education, hands-on demonstration, and training for staff in the General Units. Visitation hours are usually an issue only in ICU areas, which may explain why this non-pharmacological intervention is not often documented in General Units.
While the General Units and the High Acuity Units did not differ significantly in their use of pharmacological interventions, both units noted a lack of knowledge and awareness of delirium. Furthermore, the High Acuity Units also reported staff shortages, communication gaps between the interprofessional team, and a higher percentage of patients who are difficult to assess. Staffing shortages are a chronic problem in any healthcare facility. Thus, nurse leaders should consider strategies such as implementing telehealth nurses, incorporating behavioural health navigators, and brainstorming other ideas to help lighten the load on frontline nurses and give time back to nurses to perform critical assessments of their patients. Additional recommendations include enhancing EHR tools with hard stops that require the documentation of delirium assessment and creating policies requiring delirium assessment and documentation as part of the nursing process.
Other studies have shown that delirium is often missed in clinical care, as high as 75% of the time.13,14 Acknowledging this fact, the authors approached this project through the lens of delirium assessment compliance instead of point prevalence. As expected, the overall positive CAM screening was low amongst nurses across all specialties compared to previous studies (2-3% vs. 23 - 32%).12,15 Increased screening rates were typically associated with increased recognition.12 However, this was not the case with this project. The overall average of delirium screening performed was 64% for this study, much higher than Geriatric Medicine Research study of 24%.12 Therefore, when evaluating the delirium recognition rate, researchers must consider other factors, such as the clinician’s knowledge and whether they understand how to use the delirium screening tool appropriately. Researchers should also constantly assess the clinical tools that are part of their standard operating procedure. With the CAM tool’s known low sensitivity and implementation difficulties, hospitals should investigate the possibility of more pragmatic tools to detect delirium, such as the 4AT.16
Limitations
Several limitations to this study prevent generalising results. The small sample and cross-sectional nature of the assessment timeframes may cause assessments performed at other times during the day to be overlooked. The use of survey-based data may produce bias results, and inability to acquire participant-level data, potentially impacting data quality. Additionally, location limits the generalisation of these results to nurses’ delirium assessments at other facilities. Low CNL participation at the tertiary hospital limits CAM assessments to 5 units, affecting the true assessment compliance and recognition rates. Additionally, only CAM and CAM-ICU tools were utilised in this study. Finally, a recent transition to a new EHR limits the nurses’ familiarity and compliance with necessary documentation.
Practice Implications
Clinical implications of this work point to the need for more education and training regarding delirium assessment, interventions, and interprofessional collaboration. Delirium does not occur solely in the morning hours; hence, compliance with delirium assessment per shift and as needed is critical for early detection and intervention. Findings revealed the need for resources to help appropriately assess patients and document this assessment correctly. Assessment documentation is critical for interprofessional teammates managing the care of the patients in future shifts. Future research surrounding the use of the EHR to support compliance and documentation of delirium would provide insight into how nurses can be better supported in an assessment that is known to be difficult, further highlighted in this study.
Future studies should also explore the clinical practice differences between the two types of units. Here, the High Acuity Units experienced a higher percentage of positive CAM assessments. Interestingly, the use of non-pharmacological interventions and the barrier of personnel shortages were noted within the High Acuity Units compared to the General Units meaning that while High Acuity Units noted staffing barriers, they still used more non-pharmacological interventions than the General Units. Could staffing issues or acuity levels contribute to the differences between the two-unit types?
CONCLUSION
The findings of this project call for the need to educate bedside nurses about delirium assessment, focusing on using CAM and non-pharmacological interventions. Additionally, the results provide insight into how nurse leaders can help promote delirium prevention by providing resources to overcome existing barriers. Finally, subsequent projects should focus on ways to optimise CAM use by leveraging technology to improve the identification and prevention of delirium.
CONFLICT OF INTEREST
All authors declare that they have conflict of interest.
ACKNOWLEDGMENTS
Thank you Sharon Hood, Janice Sills, Elizabeth Anderson, Rachel Topper, and Lane Branch for assisting with data collection. We appreciate the PIs of the World Delirium Awareness Day for the opportunity to be a part of the WDAD Point Prevalence study.