INTRODUCTION
Dementia is an umbrella term for a variety of neurodegenerative diseases that cause progressive decline in cognitive function and activities of daily living, whereas delirium is transient (usually reversible) confusion caused by a physiological disturbance secondary to a medical condition, drugs and/or psychological stress.1 Both dementia and delirium are seen frequently in older hospital inpatients. Dementia is present in up to one-third of hospital inpatients aged over 70,2,3 and delirium also occurs in around one-third of older hospital inpatients, often alongside dementia. Both diagnoses are often missed.2,4
Delirium shares a complex relationship with dementia.5,6 Dementia increases the risk of delirium, and delirium increases the risk of subsequent dementia,7–10 creating a vicious cycle leading to worse health outcomes and increased healthcare costs. Potentially preventable adverse outcomes include longer length of stay, higher readmission rates, higher mortality, and more admissions to care homes.8,9,11–15
There has been very little research around the prevalence and outcomes of delirium and dementia in New Zealand (NZ) hospital settings. In a small consecutive sample (n=200) of NZ hospital inpatients aged 75+,16 40% of patients screened positive for delirium and/or dementia, half having either delirium or dementia and half having delirium superimposed on pre-existing dementia. After adjustment for age, gender and ethnic group, people who screened positive for delirium (with or without dementia) had double the length of stay and a two-fold risk of death at one year compared to patients who screened negative for both. The sample size was too small to examine ethnic differences; however, we might expect delirium to be more common amongst Māori and Pasifika people who, compared to NZ Europeans, have a higher prevalence of dementia17 and live longer with dementia,18 and therefore might be at higher risk of delirium.
Our current study aims to describe the association of dementia and delirium with health outcomes in a larger sample of patients from a New Zealand hospital setting. This will enhance statistical power and may allow stratification by major NZ ethnic groups to examine potential health disparities. We will examine total length of stay, mortality, and care home placement by diagnostic group (dementia and/or delirium versus neither diagnosis).
METHODS
Setting and sample
The de-identified data were extracted from routinely collected data from a consecutive sample of community-dwelling older patients assessed by the Memory Service at Te Whatu Ora Counties Manukau, spanning 2013 to 2021. Approximately half of assessed patients were diagnosed with dementia, and half did not have dementia. The memory service primarily accepts referrals from primary care providers and some secondary care services, excluding individuals already residing in residential care. To meet the criteria for referral to the memory service, patients must have a primary concern related to subjective and/or objective cognitive decline.
Measurements
Dementia diagnoses, including subtypes and severity, were established through clinical consensus during weekly multidisciplinary team meetings at the memory service. These diagnoses were based on a combination of clinical information and neuroimaging findings. The diagnostic criteria used for dementia followed DSM-5 guidelines,1 while the severity of dementia was assessed using the Clinical Dementia Rating (CDR) criteria.19 The Confusion Assessment Method or CAM20 is a questionnaire that screens for delirium. It can be completed within five minutes and is based on four features: acute onset and fluctuation course (i), inattention (ii), disorganised thinking (iii) and altered level of consciousness (iv). The delirium diagnosis requires the presence of features (i) and (ii) as well as either (iii) or (iv).
Data collection
Routinely collected data extraction included age, gender, ethnicity, CAM scores and dates, hospitalisation data, care home placements and mortality data. We defined delirium as scoring positive on all four CAM questions at least once during any hospital admission after they were assessed for dementia. CAM was scored on routine clinical observation. Systematic delirium screening was introduced in the hospital for patients aged 65+ quite recently, so full coverage has not yet been achieved. Initial and updated diagnoses of dementia were routinely collected. Subsequent delirium episodes were considered after the updated dementia diagnosis for those who had it. For patients without dementia, given the characteristics of the data, we assumed they did not change in the diagnosis.
Statistical analysis
All data were de-identified before analyses. Patient ethnicities were categorised as NZ European, Māori, Pacific Islander, and other (although people of Chinese and Indian ethnicity are major ethnic groups in NZ, the numbers in our data did not warrant a separate category). We created four diagnostic categories regarding dementia and delirium: delirium only, dementia only, dementia and (at least one episode of) delirium, and no delirium/no dementia. Baseline characteristics between groups were compared using the chi-squared test, Fisher’s exact test, student t-test, Mann-Whitney U test, analysis of variance (ANOVA), and Kruskal-Wallis test. Logistic and multivariate Cox regression were carried out to determine the relationship between diagnostic category, mortality, care home placement and sociodemographic variables. A generalised additive model for location, scale and shape with generalised gamma response was used to analyse the association between diagnostic category and length of stay because it tolerates skewed data. We used a level of significance of 5%. All statistical analyses were made using statistical software R 4.3.1 version.21
RESULTS
Between 2013 and 2021, 2248 patients underwent clinical evaluations for dementia at the Memory Service. Approximately 56% of the sample were given a diagnosis of dementia. Diagnoses for the remainder were as follows: mild cognitive impairment (20%), psychiatric disorder (6%), medical disorder (6%), no diagnosis given (11%), and incomplete assessment (1%).
Of 2248 patients assessed, 1673 (74.4%) were hospitalised at least once during the nine-year follow-up period. Supplementary Table 1 presents the characteristics of the 1673 hospitalised patients screened for delirium (n=798, 47.7%) and those not screened for delirium (n=875, 52.3%) during any hospital episode. There were no differences in ethnicity or gender by screening status. Patients who were screened were older had a higher number of admissions and more days in hospital per person-year (which also gave them more opportunities to be screened). As universal coverage for delirium screening had not yet been achieved in the hospital, we tested whether dementia status increased the likelihood of being screened for delirium and found that it did not (p=0.712).
Association between dementia and delirium
Of the 798 patients who were hospitalised and screened at least once for delirium, 538 had dementia, 257 did not have dementia, and three did not receive a diagnosis due to incomplete assessment. Of the 795 who had a full dementia assessment and a delirium screen, 213 (27%) screened positive for delirium, and 178 (84%) of these also had dementia. A logistic regression was fitted to assess which sociodemographic and clinical characteristics were associated with delirium, see Supplementary Table 2. Due to their collinearity with number of delirium screens per person-year, total days in hospital per person-year and number of admissions per person-year were not included in the model. The number of delirium tests was included in the model to ensure that the occurrence of delirium did not have a confusing effect with the number of delirium screens since it was expected that patients with a greater number of screens would have a high probability of delirium.
We found that age and gender were not associated with delirium. On unadjusted analysis, we found that Māori were less likely to screen positive for delirium. In contrast, Pacific peoples were more likely to screen positive. Still, these findings were no longer statistically significant when they were adjusted for dementia status, gender, age, and number of delirium screens per person-year.
A diagnosis of dementia increased the likelihood of delirium three-fold. Compared to individuals without delirium, we found that each extra delirium screen increased the chance of being screened positive by 30%, and we adjusted for number of delirium screens per person-year, but this made no difference to the associations between dementia and delirium, adjusted OR=3.0 (95% CI:2.0-4.6).
Diagnostic category, sociodemographic characteristics and clinical outcomes
We divided the screened sample into four diagnostic categories based on their initial dementia assessment and whether they had screened positive for delirium at least once during the period of follow-up: delirium only (n=35), dementia only (n=360), delirium and dementia (n=178), and no delirium/no dementia (n=222). Table 1 shows the association between diagnostic category, sociodemographic characteristics, and clinical outcomes. As might be expected, older patients were more likely to have a diagnosis of dementia and/or delirium.
There was an association between diagnostic category and ethnicity: Pacific patients had a higher frequency of delirium and/or dementia than other ethnic groups, whereas Māori had a lower frequency. The adjusted relative risk ratio of having dementia only or delirium superimposed on dementia, compared to those with neither, was 2.3 (p<0.001) and 2.9 (p<0.001) in Pacific people compared to NZ European. However, the adjusted risk ratio for delirium superimposed on dementia remained lower for Māori (RR=0.46, p=0.021) compared with NZ Europeans.
Association between diagnostic category and length of stay, care home placement and mortality
Table 2 presents the association between diagnostic category and length of stay, care home placement, and mortality over the nine-year follow-up period.

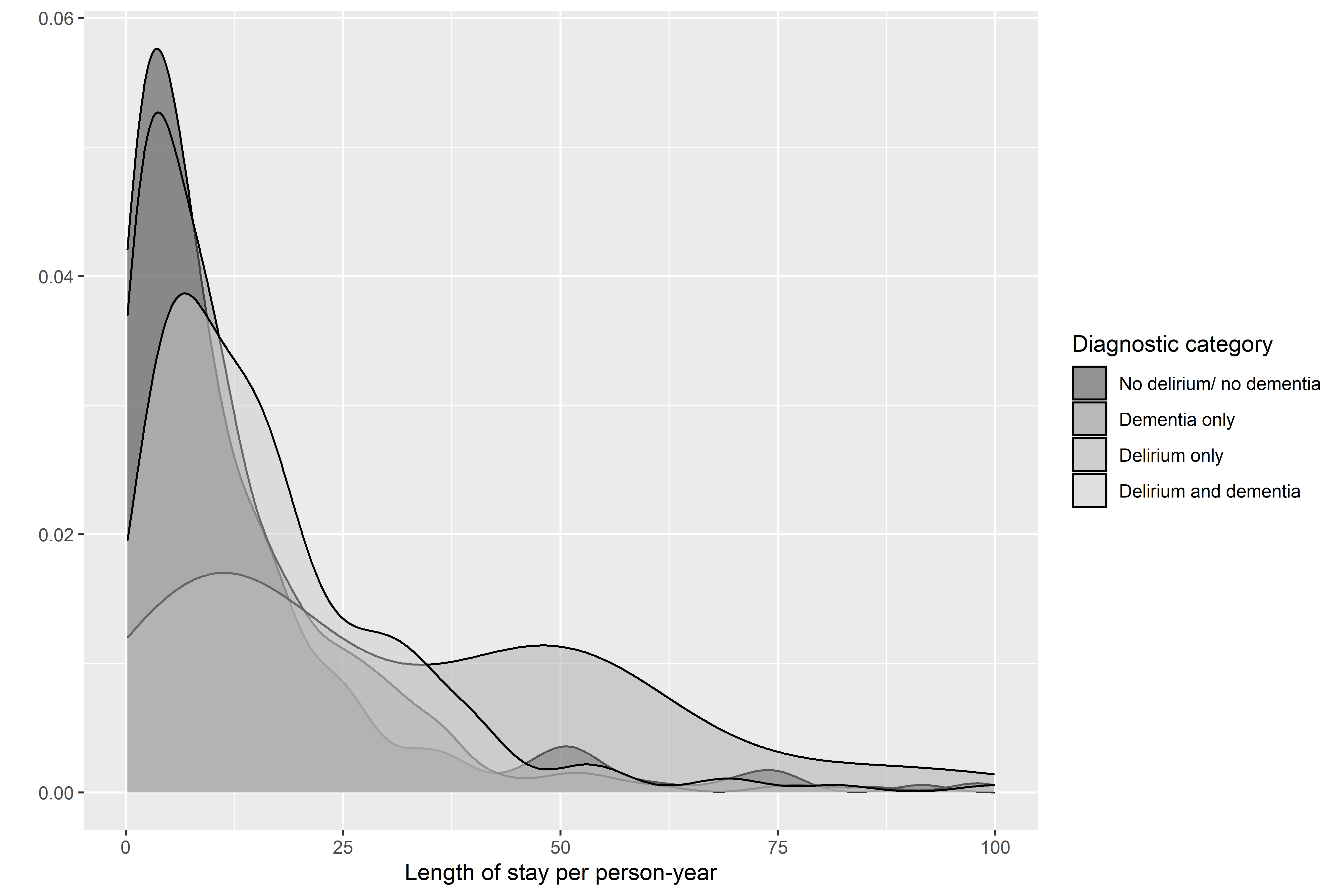
Length of stay: Supplementary Figure 1 shows the total length of stay per person-year by diagnostic category. When patients were discharged to a care home, this was associated with longer length of stay, so we adjusted the final model for care home status. After adjustment for age, sex, ethnicity and hospital discharge to care home, Table 2 shows that the mean total length of stay per person-year for patients with delirium was 2.6 times higher compared to patients without delirium or dementia (p<0.001) and 1.3 times higher in patients with both delirium and dementia (p=0.044) whereas having dementia only did not make a difference to length of stay.
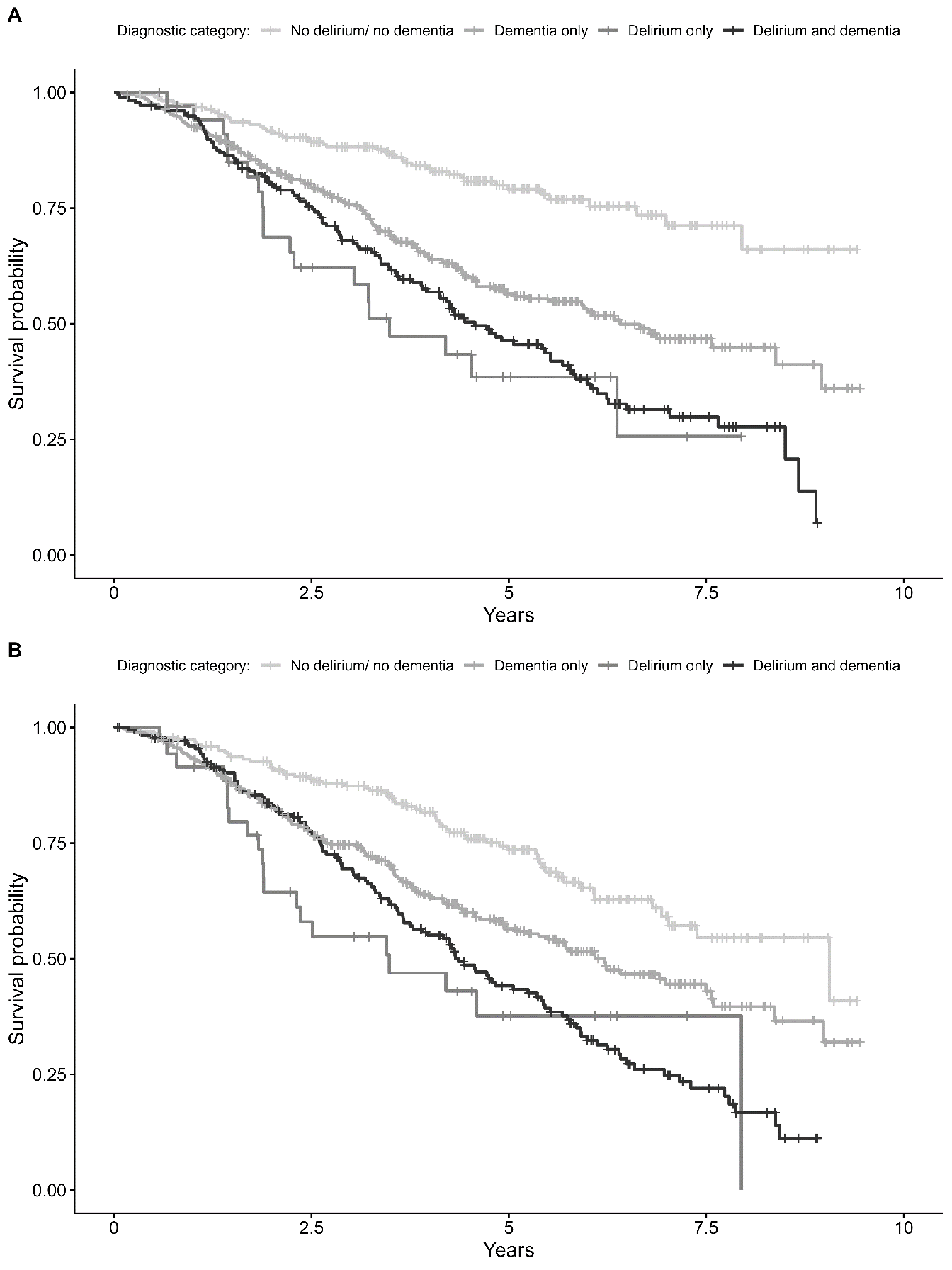
Care home placement: Figure 1 shows the Kaplan–Meier survival curve for care home placement by diagnostic category. After adjustment for age, sex, and ethnicity, Table 2 shows that patients with dementia and/or delirium had two to four times the risk of care home admission compared to patients with neither diagnosis (p<0.001).
Mortality: Figure 1 shows the Kaplan–Meier survival curve for mortality by diagnostic category. Patients with delirium only had the lowest probability of survival, followed by those with delirium and dementia (p<0.001). After adjustment for age, sex, and ethnicity, patients with delirium (with or without dementia) had a three-fold higher risk of death, whereas patients with dementia only had a 70% higher risk of death compared to patients with neither diagnosis.
Ethnicity: We were unable to test for interaction between diagnostic category, ethnicity and outcomes due to small sample size.
DISCUSSION
In our sample of 2248 patients who had been assessed for dementia at a memory service in a New Zealand hospital, approximately 75% were hospitalised at least once during the nine-year follow-up, and half of these (n=795) were screened for delirium at least once. In the sample of 795 hospitalised patients who had been both previously assessed for dementia and screened for delirium whilst in hospital, we found that a diagnosis of dementia tripled the risk of subsequently screening positive for delirium, replicating findings from various international studies which have reported that dementia or lower baseline cognition increased the risk of delirium by 2 to 5 times.5,6,9
When we categorised those who had been both hospitalised and screened, by diagnosis, we found that, compared to people with neither diagnosis, people with delirium (with or without dementia) had 1.3-2.6 times the total mean length of stay per person-year, their risk of death was three times higher and they were two to four times more likely to be placed in a care home. All outcomes were worse for people with delirium (with or without dementia) compared to people with dementia only. The first two findings for length of stay and mortality replicated the findings in our previous analysis of a smaller sample in NZ,16 in which people who screened positive for delirium (with or without dementia) had double the length of stay and a two-fold risk of death at one year. Likewise, our findings replicated those of recent international studies, which also reported that, compared to patients with no cognitive impairment, patients with delirium and delirium superimposed on dementia doubled the length of stay and increased the risk of mortality by two to three times.8,9,11–15 We found one other study11 that had examined the risk of subsequent care home placement, which similarly reported a 2-5 times higher risk of care home placement in patients with delirium (OR=2.4), dementia (OR=3.3), delirium and dementia (OR=5.0).
Our study sample was large enough to examine the effect of ethnicity on the risk of dementia and delirium. We demonstrated that Pacific Island patients had a higher risk of dementia and delirium superimposed on dementia than other ethnic groups. This is a new finding and is likely to be due to the higher prevalence of chronic disease and associated higher risk for dementia/delirium in Pacific Islanders17 compared to NZ Europeans. The finding may be relevant to other specific ethnic groups with higher prevalence of modifiable risk factors for dementia (and, therefore delirium). The finding that Māori had a lower risk of delirium superimposed on dementia was unexpected as Māori also have a higher prevalence of comorbidity and consequent dementia/delirium – the finding may be due to the very small sample size and requires further investigation in a larger sample.
Strengths and limitations
The main strength of our study is that every patient had a thorough diagnostic assessment through the memory service, ensuring good case ascertainment of dementia. Due to the use of routinely collected data, we were also able to include everyone who had a delirium screen, whereas participants who are too unwell to consent to participate may be excluded in prospective studies. Along with other previous studies,10,14 have shown that we can use routinely collected data to replicate the findings from similar prospective cohort designs,5,9,11–13,16 which, although not as methodologically rigorous, demonstrates the utility and cost-effectiveness of this study method.
There are three major limitations of the study. First is the incomplete ascertainment of delirium status as only half of the hospitalised patients were screened, despite hospital policy being that delirium screening should be conducted on all inpatients aged 65+. However, patients with dementia diagnoses in our sample were no more likely to be screened for delirium than those without dementia (p=0.71), which we believe demonstrates there was no selection bias that might have explained the association of delirium with dementia. Secondly, we defined delirium as a CAM score of 4, whereas, depending on which items are endorsed, some people with delirium will have a CAM score of 3; therefore, we may have underestimated the number of people with delirium in our sample. Moreover, CAM was scored on routine clinical observation; we did not score it based on answers to a structured cognitive assessment, as suggested by Inouye et al. (2001).22 The CAM has also yet to be validated in New Zealand, specifically in the culturally diverse populations in the study. Given cultural differences and especially linguistic difficulties, delirium screening tests may misdiagnose people of non-English speaking background. The third limitation is that we were unable to measure whether delirium was an independent predictor of adverse outcomes or whether its impact was mediated by physical comorbidity, functional status, and/or frailty, all of which are associated with length of stay, mortality, length of stay and care home placement. However, those previous studies that adjusted for physical comorbidity, functional status, and/or frailty could still show an independent effect of delirium.9,12,13,15
In addition to measuring potential mediators/confounders in future studies, we recommend using the 4AT as the delirium screening tool, as this has been shown to have better diagnostic accuracy for delirium than the CAM.23,24 Future research might also focus on interventions to prevent or reduce the impact of delirium, focusing on a culturally diverse population like New Zealand. Routine screening in hospitals has been shown to improve identification rates of delirium and dementia, and interventions in hospitals and care homes have been shown to be effective in preventing up to 40% of delirium (e.g., the Hospital Elder Life Program,25).
CONCLUSIONS
Delirium is very common in older hospital inpatients and has a major impact on patient outcomes and health costs, as well as being a preventable cause of dementia. Pacific Island patients had a higher risk of delirium superimposed on dementia than other ethnic groups, possibly due to higher comorbidity. Further research and service development is required to prevent or reduce the impact of delirium to improve patient outcomes and reduce health costs.
Acknowledgements
The authors acknowledge the service users of Te Whatu Ora Counties Manukau memory service and the Health Informatics Department, who extracted the health data requested for this study.
Author Contributions
CGP and SC designed the study. CGP, SY and BO extracted and de-identified the data. CGP carried out the statistical analysis. CRR supervised the statistical analysis. CGP, SC, and EG wrote the first draft of the manuscript. GD, DW, SY and CRR reviewed subsequent versions of the manuscript. All authors participated in the review of the final version of the manuscript and approved the publication.
Ethics statement
This research was approved by the Health and Disability Ethics Committee (HDEC) reference: 17/NTB/191.
Funding sources
Health Research Council New Zealand through the Health Sector Research Collaboration Grant (Te Whatu Ora Counties Manukau) HRC#20/1182.
Declaration of Interests
Authors declared no conflicts of interest.
