Introduction
Delirium and dementia are two distinct, complex and interconnected conditions in older adults,1 which present with behavioural symptoms.2 SIGN guidelines for delirium3 and NICE for dementia4 restrict antipsychotic usage only for psychosis, agitation, with either severe patient distress or risk of violence to themselves or others or if non-pharmacological treatments are ineffective or inappropriate. The various guidelines advocated the avoidance of antipsychotics in Lewy body dementia and Parkinson’s disease and regular medication reviews to assess efficacy, adverse effects and continued need for antipsychotic medication.3–6 Despite concerns regarding potential harm, antipsychotics are commonly used in acute hospital settings for delirium7–9 and dementia.10,11 A qualitative descriptive study7 found patient safety as the most influential factor for antipsychotic prescribing decision-making for acute hospital settings.
Hyperactive presentations in delirium add to workload pressures for nursing staff,12 necessitating antipsychotic medications.13 Patients referred to mental health liaison service might have a more severe delirium,14 psychotropic prescribing challenges stem from balancing medication and patient safety risks of violence or distress. A debate publication15 on delirium in complex presentations with distress or risks concludes that complex solutions are warranted and calls for robust research in clinical settings delineated according to sub-type, settings, age, and comorbidity.
The scientific literature on medication review on potentially inappropriate medications16–18 guides prescribing practice in delirium and dementia, and the STOPP/START19 for older adults, we need robust research studies on reducing agitation and distress in complex presentations in delirium and dementia. There appears to be a paucity of research on psychotropic prescribing processes for medication review in patients with severe behavioural symptoms of delirium and dementia, which the current quality improvement study attempts to address. We hypothesised that implementing medication safety standards into medication review would improve psychotropic prescribing processes and practice in delirium occurrence and dementia without delirium in a mental health liaison older adult setting. The Model for Improvement20,21 was the study’s quality improvement framework.
Our primary aim was to improve and achieve 100% clinical documentation of psychotropic medication reviews against defined medication safety standards in patients admitted to the geriatric wards with delirium and dementia without delirium and referred to the geriatric psychiatry liaison service. The secondary aim evaluated any reduction in psychotropic medications as defined by medication safety standards by comparing pre-and post-assessments.
Methods
Study Design
A quality improvement study21–23 with a time frame of 12 months from baseline measurement.
Setting
The study setting was Changi General Hospital, a public hospital in Singapore with over 1000 beds. The geriatric psychiatry liaison service covers geriatric wards with 116 beds for patients aged 65 and over.
The study team’s interdisciplinary members comprised the study lead geriatric psychiatrist, a pharmacist, an advanced practice nurse, two geriatricians, and an analyst. An international academic pharmacist was the study mentor.
The study psychiatrist conducts the geriatric liaison psychiatry induction for trainees, including a bedside demonstration of 4AT3 and DSM-V diagnostic criteria.24
The service receives bi-weekly electronic referrals on Monday and Thursday from geriatric teams. The electronic geriatric liaison psychiatry referral criteria are pre-defined in the electronic referral system. (Supplementary Figure 1).
The clinical diagnosis of all psychiatric disorders is made using the DSM-V diagnostic criteria.
4AT3 is the delirium detection tool in suspected delirium that is implemented hospital-wide and at liaison psychiatry assessments by the trainees. A probable delirium based on 4AT will be followed by a clinical diagnosis of delirium using DSM-V diagnostic criteria.
Trainees in psychiatry and psychologist from the geriatric psychiatry liaison team undertake comprehensive liaison psychiatrist assessments and reviews and contribute to the quality improvement interventions as the study stakeholders.
Baseline measurement (April to July 2022)
The current study builds on our earlier study on the measured anticholinergic burden in the geriatric psychiatry liaison service.25
A baseline measurement that we undertook evaluated prevailing clinical practice for implementing improvements. In April 2022, we evaluated fifty consecutive liaison psychiatry assessments of older adults among referrals from geriatric wards through prospective data collection. 50 was an achievable number for measurement, and the results showed 32 total assessments for delirium and 6 for dementia without delirium. There was no clinical documentation of whether a medication review occurred for prescribed hypnotics, antipsychotics, and psychotropic polypharmacy, and we identified the need for improvement.
PDSA and strategy for improvement (Supplementary Figure 2)
Plan-Do-Study-Act (PDSA)21–23 methodology operationalised and implemented medication safety standards and evaluated improvement.
Plan: Understanding prevailing practice and planning interventions for improvement.
Do: Testing and implementing interventions.
Study: Collecting data, evaluating interventions and analysing results.
Act: Evaluating and refining improvements through repeating PDSA for the second cycle.
Driver diagram26 (Supplementary Figure 3)
PDSA cycle 1 (September to December 2022)
The first intervention involved creating and embedding 4 medication safety standards in medication reviews. The first three medication safety standards were a review of hypnotics (includes benzodiazepines, Z drugs, and other hypnotics: antihistamines hydroxyzine and melatonin), antipsychotics, and psychotropic polypharmacy defined as ≥3 psychotropic medications. The fourth safety standard reviewed measured anticholinergic burden using the Anticholinergic Effect on Cognition (AEC) scale,25,27 a high burden defined as ≥3. Medichec,27 an online resource, calculated anticholinergic burden scores and guided psychotropic medication prescribing decisions as a decision support tool. The AEC addresses the central anticholinergic burden compared to other anticholinergic burden scales and has been implemented in the geriatric liaison psychiatry service.
SIGN3 and NICE5 Guidelines for delirium and NICE4 and Irish National Clinical Guidelines for dementia6 underpinned the inclusion of the study’s medication safety standards.
The second intervention involved the addition of headings on medication safety standards in our clinical documentation, which served as audit checklists to review psychotropic medication usage.
PDSA cycle 2 (December 2022 to February 2023)
Continual refinements to the interventions in the current quality improvement initiative led to adding a fifth medication safety standard, a blood pressure review and postural hypotension monitoring. Orthostatic hypotension has the greatest risks with polypharmacy, 28 and antipsychotics are associated with up to twice the odds of orthostatic hypotension, underpinned the scientific rationale for inclusion.
The process for medication review of medication safety standards
The medication review involved an evaluation of all psychotropics against defined medication safety standards to optimise medicine use and improve health outcomes.29
Trainees documented all team discussions on psychotropics’ benefits and adverse effects, added headings of medication safety standards in the documentation assessments and recorded whether the medication review occurred. (Supplementary material).
Medication review strategies included dose reduction, switching, changing from regular to as-needed, and deprescribing whenever appropriate. Additionally, we reviewed other delirogenic drugs: steroids and opioids and highlighted them in our documentation in both cycles.
Data collection
The study psychiatrist collected data prospectively using electronic medical records of all geriatric psychiatry liaison assessments of delirium occurrence and dementia without delirium. To ensure data accuracy, independent data verification by the study pharmacist was conducted to verify all data captured by the study psychiatrist on Excel spreadsheets.
Standard and outcome measurement for the primary aim
We evaluated whether a medication review occurred against defined medication safety standards documented at each assessment by the trainees.
The standard for documentation records for medication review was pre-determined at 100%.
Standard and outcome measurement for the secondary aim
The reduction in psychotropic medications was evaluated by comparing pre-assessments and post-assessments. The standard for improvement was not pre-determined as we compared the change from pre- to post-assessments.
Data analysis
Descriptive statistics were utilised to provide an overview of the study cohort of delirium and dementia without delirium and relevant variables. Demographic characteristics were summarised using mean, standard deviation, and percentages. The frequency and percentage distribution of psychotropic medications prescribed before and after assessments are presented.
For the secondary aim, bar diagrams were used to depict the reduction in rates of psychotropic medications in post-assessments compared to pre-assessments. Data was analysed using Microsoft Excel 2016.
Results
Study characteristics
We had 27 patients with total delirium occurrence and dementia without delirium in cycle 1 and 22 in cycle 2. More than half of the patients (59%) in both cycles had delirium occurrence, and 40% had dementia without delirium. Behavioural and mood management was the commonest referral reason in the study cohort. Patient characteristics, diagnoses and referral reasons for delirium occurrence and dementia without delirium are presented in Table 1.
Primary aim
The study’s main findings on the primary aim are summarised in Table 2.
In delirium, the defined medication safety standards for the record of review of standards 1 to 3 in assessments (hypnotics, antipsychotics, and polypharmacy) were 87.5% in cycle 1, increasing to 100 % in cycle 2.
In dementia without delirium, the review record of standards 1 to 3 in assessments was 100 % in cycle 1 and 95 % in cycle 2.
The anticholinergic drug burden medication review as the fourth standard was a 100% review record in both cycles for delirium and dementia without delirium, sustaining results from an earlier study.
The fifth additional blood pressure and postural hypotension standard added in cycle 2 showed an 87.5 % review record for delirium and 95% for dementia without delirium.
Secondary aim
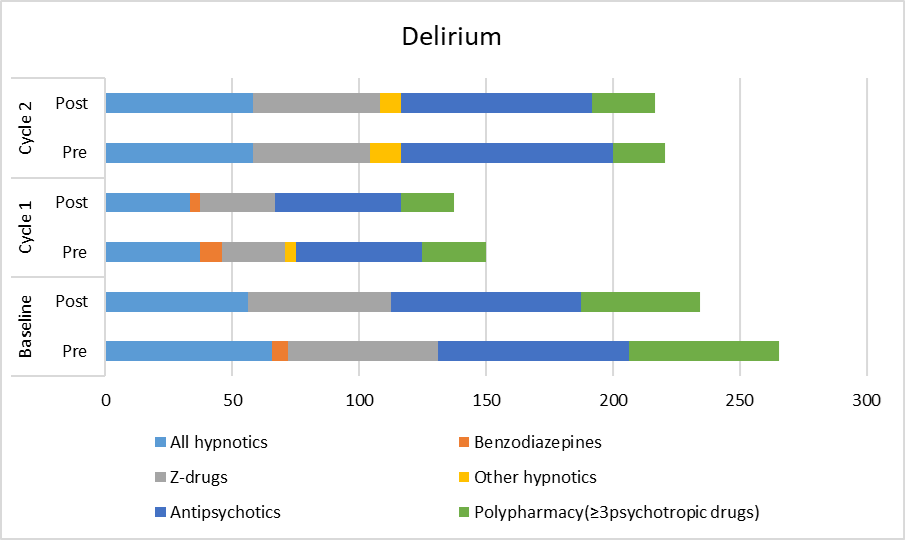
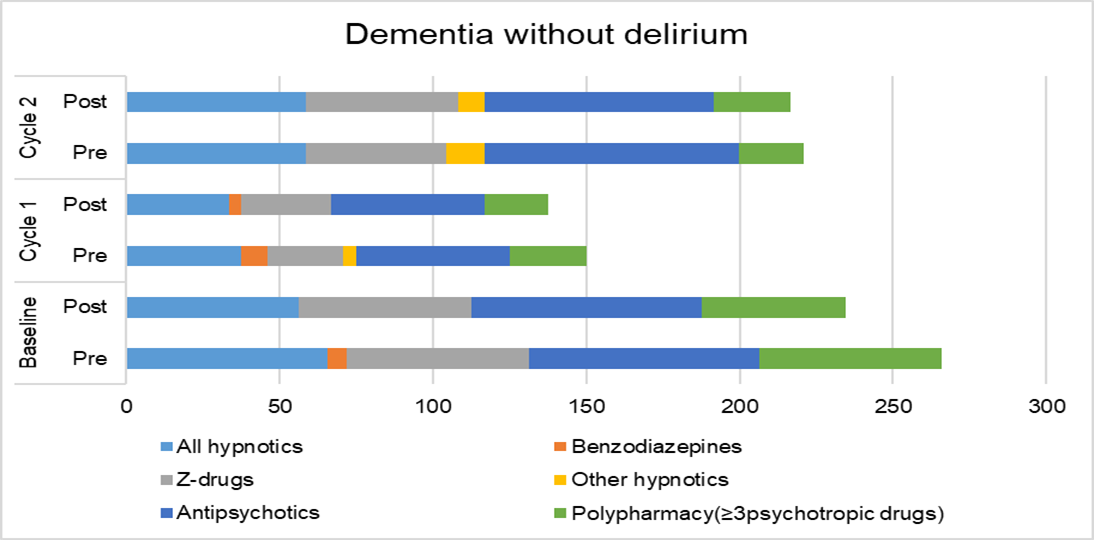
The results of the psychotropic medications prescribed are presented in Table 3, and the reduction of psychotropic medications by comparing pre-and post-assessments are in Figure 1A (delirium) and Figure 1B (dementia without delirium).


In delirium, the reduction of benzodiazepines at post-assessment compared to pre-assessment was 4.2% from 8.3% in cycle 1 and nil prescriptions in both pre-and post-assessments in cycle 2. There was no reduction for Z drugs in both cycles. For other hypnotics, there was a reduction in both cycles at post-assessment to 0% from 4.2% in cycle 1 and 8.3% from 12.5% in cycle 2. For antipsychotics, the reduction was only in cycle 2 to 75% from 83.3%. In polypharmacy, there was a reduction to 20.8% from 25.0 % only in cycle 1. High AEC scores in cycle 1 were reduced to 4.2% from 8.3%, and nil high scores in cycle 2 at pre-and post-assessments.
In dementia without delirium, benzodiazepines at post-assessment compared to pre-assessment, there was a reduction to 0% in both cycles. The reduction was in cycle 2 to 25% for Z drugs from 40%. For the other hypnotics, there was no change in cycle 1 and nil drugs at pre-and post-assessment in cycle 2. For antipsychotics, there was a reduction to 21.1% from 47.4% in cycle 1 and to 80% from 85% in cycle 2. There was a reduction to 50% from 55% in polypharmacy only in cycle 2. High AEC scores were reduced to 21.1% from 26.3% only in cycle 1.
The anticholinergic burden in both cycles was due to prescribed antipsychotics and antidepressants in single or combination. Hydroxyzine contributed to the burden scores in one case of delirium in cycle 1.
Discussions
Using a quality improvement framework that embeds defined medication safety standards as an intervention, we have demonstrated good documentation records for a medication review to improve psychotropic prescribing processes in delirium occurrence and dementia without delirium in geriatric wards. We have shown a reduction in all psychotropic medications at post-assessment as defined by the medication safety standards 1 to 4 in at least one cycle in both delirium and dementia without delirium, except for zopiclone in delirium, where there was no reduction in both cycles. For other hypnotics, in dementia without delirium in cycle 2, there were nil prescriptions at post-assessment. In cycle 2, post-assessment results showed decreased antipsychotic medications for delirium (8%) and dementia without delirium (5%). High anticholinergic burden scores for delirium were nil in cycle 2 and below 10% in cycle 1, sustaining improvement from our previous study.
A cross-sectional analysis of an Irish national pharmacy claims database for general medical services patients demonstrated a significant decline in benzodiazepine prescribing but an increase in Z drug prescriptions, consistent with our findings.30 A meta-analysis on melatonin intervention in hospitalised medical inpatients31 has shown that melatonin may reduce delirium incidence rates in medical inpatients. Therefore, clinicians must continually evaluate medications through a comprehensive review, which our study reiterates.
Our study anticipated a relatively high psychotropic polypharmacy and antipsychotic prescribing rate considering the severe mood and behavioural symptoms as common referral reasons to the liaison service. Psychotropic polypharmacy is more commonly defined32 as two or more psychotropic medications. A shift towards using the term appropriate polypharmacy is needed.33–35 A pragmatic standard for inappropriate psychotropic polypharmacy and a definition of three or more psychotropic medications were agreed upon with the study team.
The study illustrates the role of a quality improvement framework in evaluating and refining psychotropic medication prescribing in delirium and dementia in an older adult liaison psychiatry clinical service to geriatric wards. The creation and application of medication safety standards have implications for clinicians to evaluate their practice continually.
This study draws on the strengths of a multidisciplinary effective team working36 in the clinical setting. The other strengths involved developing a framework for medication safety standards and review, specifically in patients with delirium and dementia in older persons’ mental health liaison settings, to enhance prescribing processes.
Our study, however, has the following limitations. The service has restricted bi-weekly liaison referral days; therefore, potential selection bias with referrals from the geriatric team is a limitation. We acknowledge measurement bias but minimised by trainees documenting all assessments and the pharmacist verifying data collected by the study’s lead author. We did not capture records of the medication review strategies, such as dose reduction or changing regular prescriptions to as-required medication, which might have spuriously increased reported psychotropic medication prescribing rates and polypharmacy.
Whilst the results showed a psychotropic medication reduction which we have attributed to the study’s interventions, the observed medication reductions could have been attributed to secular trends over time with delirium recovery and improvement in behaviour symptoms due to response to non-pharmacological interventions we did not capture. The fifth standard in cycle 2 may have contributed to the antipsychotic reductions in both delirium and dementia in cycle 2 through increased vigilance in prescribing.
However, it was beyond the study’s scope to capture additional variables or medications over and above what we elicited. We acknowledge that the improvement in psychotropic prescribing may have been due to the possibility of chance in a small-scale study in a mental health liaison setting, which may limit generalisability as it is a referred cohort of patients. Finally, the study improved psychotropic medication prescribing processes that should link to better patient safety outcomes regarding falls, mortality and cognitive decline, which we did not measure.
Conclusions
The study’s findings from a small-scale single-centre study in a geriatric ward setting that employed a quality improvement framework support the feasibility of embedding medication review using defined medication safety standards to improve psychotropic medication prescribing processes in older adults with delirium occurrence and dementia without delirium.
To refine clinical practice, we propose the need for further robust research on the effectiveness of psychotropic medication interventions and review in reducing agitation and other patient safety outcomes in older adults with delirium and dementia with complex presentations of risks of violence and distress.
Acknowledgements
Healthcare Professionals
The authors thank Professor Robert Stewart, Professor of Psychiatric Epidemiology and Clinical Informatics, Kings College London, Department of Psychological Medicine, Institute of Psychiatry, Psychology and Neuroscience, and his research and clinical team, with whom the first author undertook an observer placement in 2019.
The authors thank all trainees, medical officers, and psychologists participating in the Geriatric Psychiatry Liaison Service provision. We thank all medical colleagues from the geriatric psychiatry service provision, Department of Psychological Medicine and Department of Geriatric Medicine, Garry Semeniano and Alvin Chew Zhen Jie, Office of Improvement Science, Changi General Hospital.
Caregiver
This Quality Improvement Project benefits from a caregiver’s involvement in the current project’s aims, rationale, medication safety and benefits to patients with delirium and cognitive impairment. We are most grateful to the caregiver Ranjini D/O Subramaniam and her consent to formal acknowledgement through a medical journal publication.
Author contributions
BB and SY conceptualised the study design.
BB wrote the first draft of the article with revisions by SY.
All authors and the mentor were involved in the study design, planning, interpretation of data and critical revisions.
MHT was the analyst.
DB supervised the study as a mentor and assisted with scientific evidence on pharmacological interventions and medication safety in dementia.
All authors have consented to the publication in Delirium or Delirium Communications.
Ethics statement
Ethics Committee: SingHealth Centralised Institutional Review Board Exemption applies to healthcare, quality and service improvement studies. SingHealth Centralised Institutional Review Board, Singapore, advises exemption from a formal application for ethical approval as this is a healthcare and quality improvement study.
Sources of study funding
None.
Declaration of conflict of interests
None.
Participant consent
Not applicable as this is a healthcare improvement study.
Author’s note
SQUIRE Guidelines have been used to craft the manuscript writing.37