Introduction
Patients in acute cardiac care units hold a high risk of developing delirium due to hardware-related immobility, cerebral hypoperfusion with a low cardiac output, status post transcatheter aortic valve replacement procedure, or status post-cardiac arrest.1 The incidence of delirium in the cardiac intensive care unit varies depending on the screening tools and methods for assessment, but it ranges between 3% and 41.7%.2,3 Multiple studies have shown that a patient-centered multicomponent approach is effective in delirium prevention and management.4–6 However, application of such multicomponent care in a fast-paced specialized care unit like a cardiac care unit, may be challenging and impractical.
Recently, the Institute for Healthcare Improvement and the John A. Hartford Foundation launched Age-Friendly Health System (AFHS) 4Ms initiative.7 The AFHS 4Ms initiative promotes a framework addressing four key components called 4Ms: “What Matters,” “Medication,” “Mentation,” and “Mobility.” The rationale of the 4Ms is that by addressing each M, any healthcare system can provide high-quality and age-friendly care for older adults. Briefly, “What Matters” stands for patient-centered care aligning care plans to what matters most to older adults, “Medication” proposes healthcare providers avoid inappropriate medications, “Mentation” promotes screening, preventing, and managing delirium, dementia, and depression, and “Mobility” promotes older adults’ physical activities and avoids immobilization.
Given that the AFHS 4Ms framework intends to promote comprehensive care strategies and addresses delirium in its “Mentation” domain, AFHS 4Ms could be used for a patient-centered multicomponent approach in delirium prevention and management. Studies have reported the importance of medication management (“Medication”) or promoting mobility (“Mobility”) in optimal delirium prevention and management. Avoiding certain medications such as anticholinergics, antihistamines, or benzodiazepines is critical in preventing delirium.8 Physical rehabilitation has immediate benefits in older adults’ mentation and management of postoperative delirium.9 However, these 4Ms have only been studied individually, and there has not been a study assessing the effectiveness of AFHS 4Ms as a whole on delirium care. Furthermore, it has not been studied if AFHS 4Ms could be successfully implemented in a specialized care unit. Therefore, we conducted a quality improvement (QI) project implementing the AFHS 4Ms focusing on delirium detection and management and assessed its feasibility in acute cardiac care units.
Methods
We applied the AFHS 4Ms framework at two acute cardiac care units, cardiac intensive care unit (CCU) and cardiac intermediate care unit (CIMU) at a tertiary academic medical center (Memorial Hermann Hospital at Texas Medical Center) in Texas, U.S.A. These two units did not have a formal delirium screening process before the QI project, so we focused on delirium detection and proper management using the AFHS 4Ms framework and assessed its feasibility.
The 4Ms implementation
One of the AFHS 4Ms’ strengths is that it allows any healthcare system to build a specific strategy for each M depending on their goals and resources, as long as the strategy meets the minimum requirement outlined in the guideline.10 Therefore, AFHS 4Ms are versatile and site-specific. Since we believed that the feasibility and effectiveness of such site-specific 4Ms strategies should be tested in a relatively small unit, we chose to conduct this project at CCU and CIMU rather than at the entire hospital.
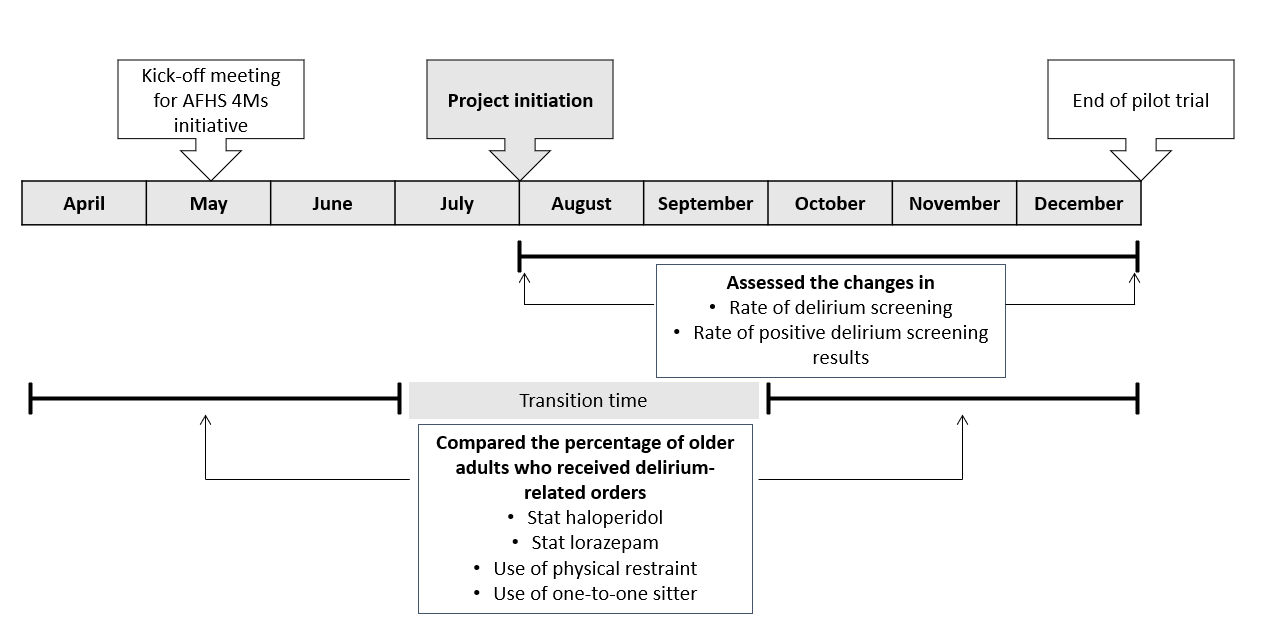
The initial planning meeting was held in May 2019 with a multidisciplinary team, which included a geriatrician, a nurse manager, and a nurse educator. The team discussed overall goals and site-specific strategies. From May to August 2019, the team finalized specific strategies for all 4Ms and started the implementation in August 2019 (Figure 1). During the QI project, a geriatrician attended the daily multidisciplinary meeting to ensure that AFHS 4Ms were implemented and to address any questions or concerns from the staff. Our site-specific strategy for each M is described below.
-
For the “What Matters” domain, the bedside nurse asked the patient, “What matters most to you today?” and reported it during the daily multidisciplinary meeting so the team could be aware of the patient’s priorities and take those into account.
-
For the “Mentation” domain, we educated the nurses in screening for delirium using the Brief Confusion Assessment Methods (b-CAM)11 if the patient was not intubated, and Confusion Assessment Methods – Intensive Care Unit (CAM-ICU)12,13 if the patient was intubated. We provided two educational sessions to train the nurses in using b-CAM and CAM-ICU. Additionally, a geriatrician attended the daily multidisciplinary meeting during the QI project to provide feedback on their screening skills. Then the nurses recorded the results in the electronic medical record and also reported the results during the daily multidisciplinary meeting. We provided reading glasses and hearing amplifiers for older adults if needed. For better reorientation and to avoid frequent naps during the day, we provided puzzles and word-search books that they can use for their entertainment.
-
For the “Medication” domain, we already had a built-in system in the electronic medical records to warn the prescribers when they are about to order potentially inappropriate medications based on the American Geriatrics Society’s Beer’s Criteria.14 Furthermore, for this project, the pharmacists designated for the units received a list of potentially inappropriate medications so that they could inform the prescriber to consider discontinuing that medication. This is an extension of their routine practice of supervising medication utilization.
-
For the “Mobility” domain, we had the nurses assess the patient’s ambulation by direct observation of patient’s gait to determine any possible needs for physical assistance even prior to the official physical therapy evaluation was performed. If the patient needed physical assistance, the nurses prompted the physicians to order formal physical therapy assessment. We provided the units with additional walkers and canes so that older adults could use during their hospital stay and hence improve their chances of ambulation.

Data collection
The CCU and CIMU are on the same floor and admit patients with cardiologic conditions or receiving a cardiologic intervention. Patients are transferred easily between the two units, so we combined the data from the two units. We included all older adults (≥ 65 years old) admitted to the two units. Since the project was a QI project focusing on the feasibility of the AFHS 4Ms implementation, we did not apply any other specific exclusion criteria other than age. Furthermore, we reported the results in aggregated form without collecting the patient’s other individual data. The current project received approval for QI project from both the University of Texas Health Science Center and Memorial Hermann Hospital. Therefore, we were waived from requiring informed consent.
Outcomes
The primary outcomes were the changes in monthly delirium screening rate and positive screening rate over time during the project. The monthly delirium screening rate was calculated as the number of older adults who were screened for delirium using b-CAM or CAM-ICU during the month/ number of older adults who were admitted to the two units during the month. The rate of positive delirium screening results was calculated as the number of older adults who had positive results from b-CAM or CAM-ICU during the month/ number of older adults who were screened for delirium during the month.
The secondary outcomes were delirium-related orders, including a stat haloperidol order, stat lorazepam order, physical restraint order, and one-to-one sitter order. Since our units were not screening for delirium before the initiative, we could not compare the prevalence or incidence of delirium before and after using the screening rate. Therefore, we chose these secondary outcomes as the proxy for assessing delirium management to compare before and after the initiative. We selected the four orders frequently used for delirium management in our units after a discussion as a team. To capture their use for urgent situations and minimize including those taking them as home medications, we only included orders prescribed as “stat.” For these secondary outcomes, we compared the percentages of older adults who received the four orders (number of older adults who received the order/ number of older adults who were admitted to the two units) before the initiative (April ~ June 2019) and after (October ~ December 2019). We did not use the data from July 2019 to September 2019 because that was a transition and dissemination period.
Statistical Analysis
Although the main purpose of this project was to assess AFHS 4Ms’ feasibility, we conducted a statistical analysis to assess the changes in the rate of screening and the rate of positive screening results over time (primary outcomes) using Cochran-Armitage test for trend and Fisher’s exact test for comparison of the delirium-related orders (secondary outcomes) before and after the initiative. Statistical significance was defined as p-value <0.05.
Results
Primary outcomes
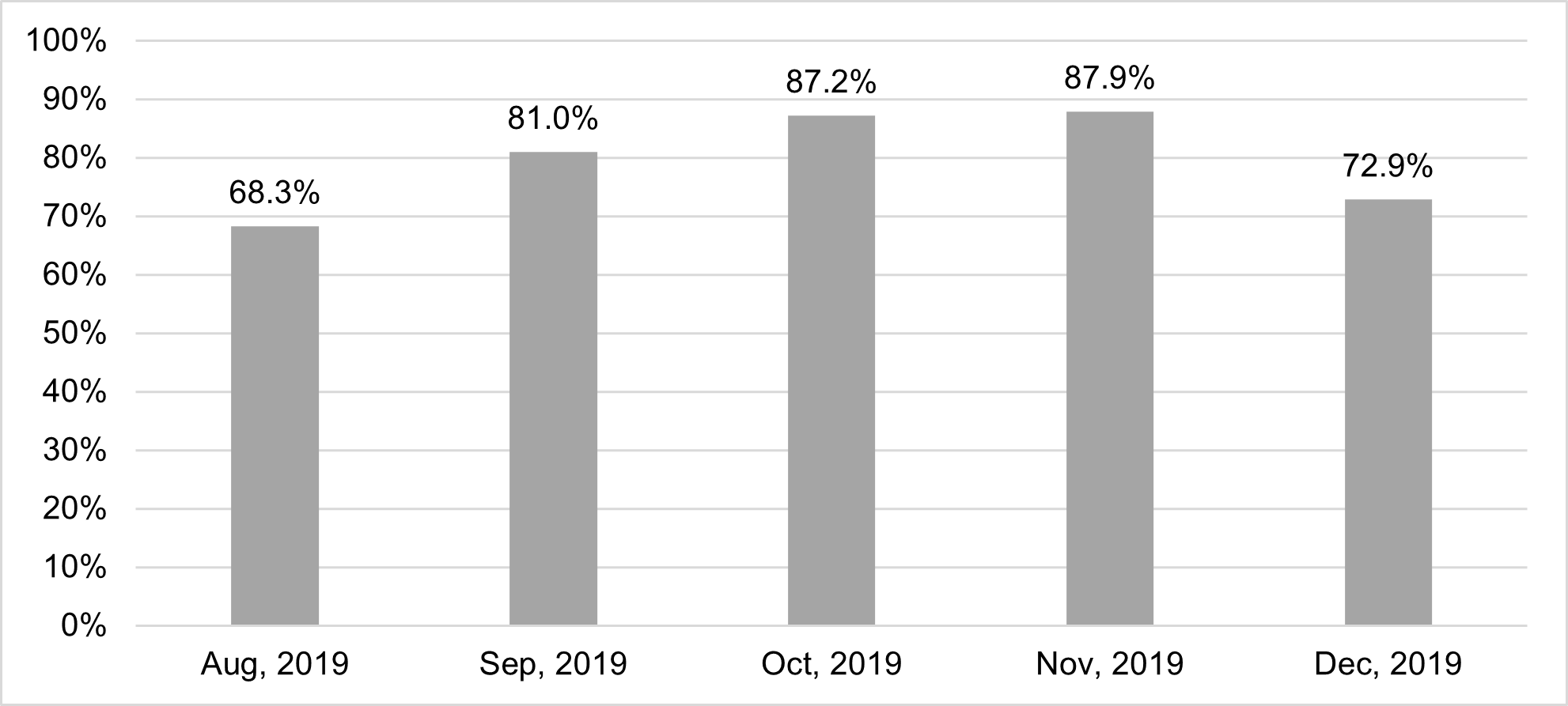
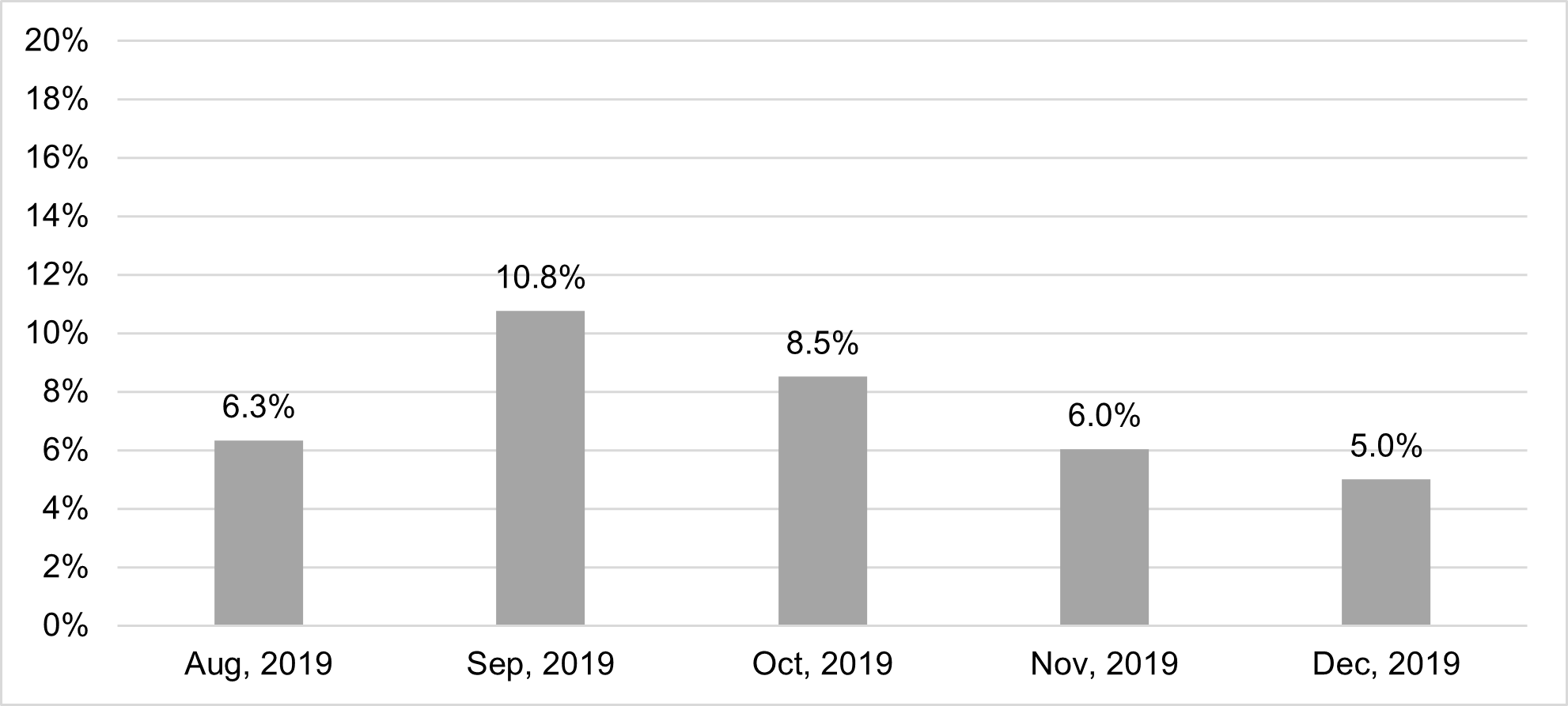
During the project period, 730 older adults were eligible to receive AFHS 4Ms care. In August, the delirium screening rate was 68.3% (97/142). It increased to 81.0% (128/158) in September, 87.2% (123/141) in October, and 87.9% (131/149) in November but slightly decreased to 72.9% (102/140) in December. The p-value for a trend was non-significant (p=0.230). The overall screening rate during the project period was 79.6% (581/730) (Figure 2). The rate of positive delirium screening results was 6.3% (9/97) in August, increased up to 10.8% (17/128) in September, but declined to 8.5% (12/123) in October, 6.0% (9/131) in November and 5.0% (7/102) in December (Figure 3). The p-value for a trend was non-significant (p=0.162). The overall rate was 9.3% (54/581).


Secondary Outcomes
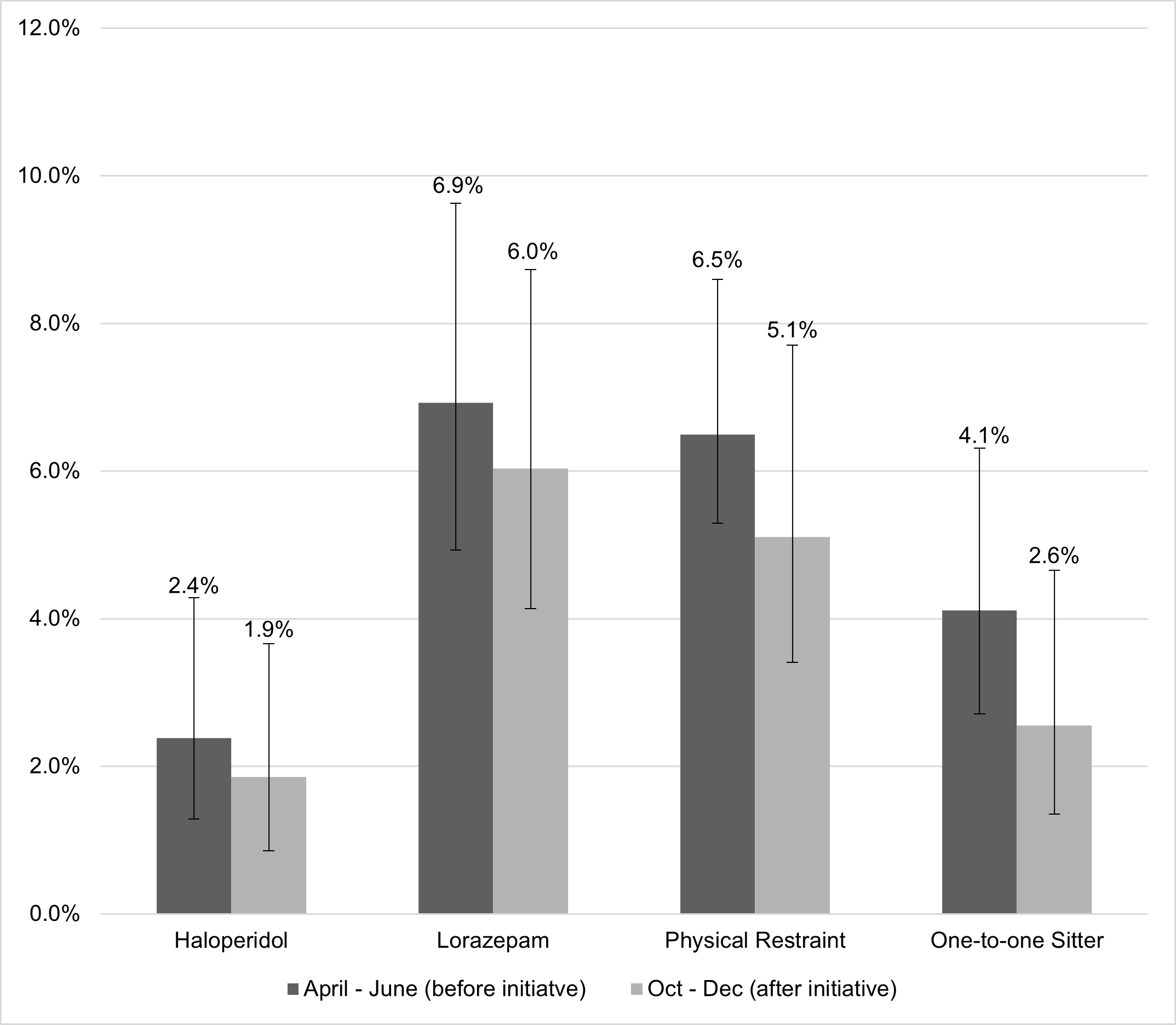
We compared the secondary outcomes (the percentage of older adults who received delirium-related orders among all of the older adults admitted in the two units) before the initiative (April ~ June) versus after the initiative (October ~ December). A total of 462 older adults from April to June and 430 older adults from October to December were included in the data analysis. In the before group, 11 (2.4%) older adults received haloperidol stat orders, 32 (6.9%) received lorazepam stat orders, 30 (6.5%) received physical restraint orders, and 19 (4.1%) received one-to-one sitter orders. In the after group, 8 (1.9%) older adults received haloperidol stat orders, 26 (5.1%) received lorazepam stat orders, 22 (3.0%) received physical restraints, and 11 (2.6%) received one-to-one sitters. Overall, the results showed trends of reduced utilization of all delirium-related orders, but they were statistically insignificant (Figure 4).

Discussion
In this article, we report the results from a QI project applying AFHS 4Ms focusing on detecting and managing delirium in acute cardiac care units at a tertiary academic medical center. To our knowledge, this is the first study reporting the feasibility of AFHS 4Ms as a whole focusing on delirium detection and management. The high rate of delirium screenings administered authenticates the feasibility of the application of AFHS 4Ms in acute cardiac care units. Furthermore, although it was not statistically significant, the results showed a decreasing trend in the rate of positive delirium screening results over time.
One important aspect of the current study is that it showed that AFHS 4Ms are interconnected. The main concept of AFHS 4Ms7,15,16 is that 4Ms are not mutually exclusive but are closely related and must work together to fulfill “What Matters.” Furthermore, AFHS 4Ms are specifically built so that addressing one M can assist in addressing another M simultaneously. For example, we observed reduced rates of prescriptions for potentially inappropriate medications,17 lorazepam and haloperidol, addressing the “Medication” domain, although our main focus was “Mentation.” Furthermore, we observed reduced use of physical restraints, which can potentially improve older adults’ “Mobility.” Physical restraint is one of the risk factors of immobilization,18 and in turn, immobilization is one of the precipitating factors of delirium.19
Although this QI project taught us the important aspects of 4Ms that are feasible to be implemented in acute cardiac care units holding its main concepts as stated above, it did not demonstrate significant changes in both primary and secondary outcomes. The rate of screening for delirium did not significantly increase during the study period. However, given that our units were not screening for delirium before the initiative, achieving an overall 79.6% of screening rate in four months can be considered a success. Regarding the rate of positive delirium screening results, it did not show a significant decrease over time. One of the explanations could be due to the short study time. Another explanation is that we did not deliberately evaluate the accuracy of CAM among the older adults in our cardiac care units, as well as with our nursing staff. Indeed, the accuracy of CAM screening is highly dependent on the training level of the performer.20 Additionally, not excluding older adults with dementia in our analysis may have also affected the results. Our results showed relatively lower rates of delirium than other studies, possibly due to the inaccuracy of the screening, but also due to the confounding effect of the population with dementia. Nurses may have attributed “confusion” to dementia, not recording it as delirium on superimposed dementia.21,22 Regarding the delirium-related orders, they were not significantly different before and after the initiative. We believe it is because we did not apply strict inclusion and exclusion criteria in selecting the delirium-related orders. Certainly, there are many other conditions that the four orders can be used, and also there are other orders that can be used for delirium management. Future studies with more accurate delirium screening tools for the specific population and more comprehensive outcome measures to capture appropriate delirium management are needed to fully assess the impact of AFHS 4Ms on delirium prevention and management.
The authors acknowledge that our QI project has several limitations. First, our QI project does not compare the screening rate and positive screening results before and after the initiatives but only shows the changes after the initiative was implemented. Second, to overcome the above-mentioned limitation, we used secondary outcomes as the proxy of delirium to indirectly compare the incidence of delirium before and after the initiative. However, we acknowledge that they are not a comprehensive list since other medications are frequently used for delirium. Third, although b-CAM and CAM-ICU are well-validated tests for screening for delirium, it requires training and education for accurate assessment. Their accuracy and inter- and intra- rater reliability in our unit were not assessed. Furthermore, positive screening results from CAM may not warrant the diagnosis of delirium since CAM is a screening test, not a diagnostic tool. Fourth, we only collected the data for five months after the QI project. Although we continued AFHS 4Ms in our units, data collection was heavily impacted by the COVID-19 pandemic, and unfortunately, we only had the data available until December 2019. Fifth, our QI project was conducted in a specialized cardiac care unit, which should be tested in other healthcare settings for better generalizability. Last, we also do not have sufficient data regarding the most important domain in AFHS 4Ms, the “What Matters” aspect, although patient-centered care is also critical in delirium management.
Despite several limitations, our QI project holds significant value. As the first report assessing the feasibility of applying AFHS 4Ms in delirium care, the results of our study suggest that it is feasible to implement AFHS 4Ms in highly specialized and fast-paced cardiac units. Future prospective studies with longer study periods and more detailed outcome assessments are strongly warranted.
Acknowledgment
The current QI project results have also been presented during webinars of the Institute for Healthcare Improvement, 2022 American Delirium Society Annual Conference, and as a part of a blog posting of the Institute for Healthcare Improvement (https://www.ihi.org/communities/blogs/improving-care-while-dramatically-reducing-costs). The authors deeply appreciate the late Dr. Carmel Dyer for the inception of the current project and her life-long devotion to the field of geriatric medicine.
Author Contribution
MK – project administration, data curation, formal analysis, and writing (original draft); MJ – project administration, supervision, data curation, and writing (review and editing); CM, KY, JA – supervision, data curation, and writing (review and editing); NA- supervision and interpretation of statistical analysis and writing; PB, MW – supervision and writing (review and editing)
Ethics Statement
The current project received approval for quality improvement from both the University of Texas Health Science Center and Memorial Hermann Hospital.
Funding Sources
Not applicable
Declaration of Interests
Dr. Kwak receives a consult fee from the Institute for Healthcare Improvement.